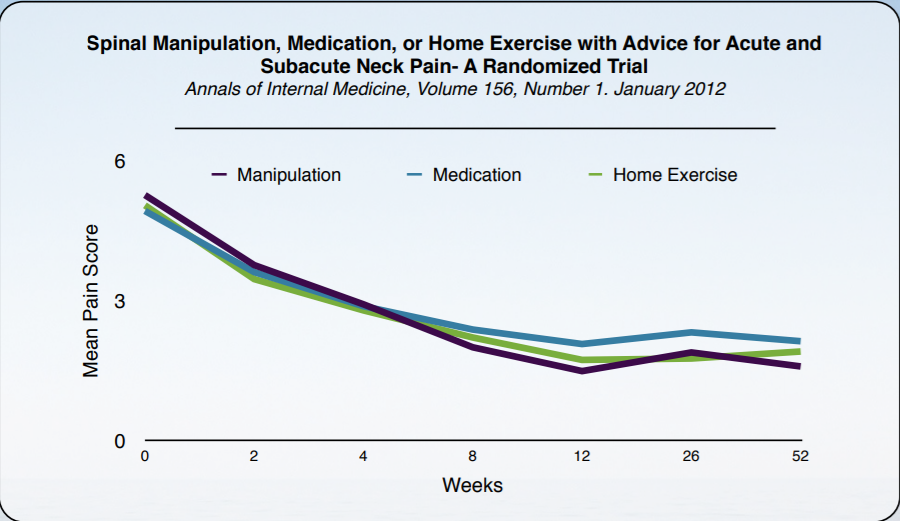
Summary of “Spinal Manipulation, Medication, or Home Exercise with Advice for Acute and Subacute Neck Pain- A Randomized Trial Annals of Internal Medicine, Volume 156, Number 1. January 2012”
Common treatments for neck pain are medication, exercise and spinal manipulation. This 2012 study compares spinal manipulation to medication (acetaminophen, NSAID’s, muscle relaxants, or narcotics) and home exercise/advice in patients whose average age is 48 years old.
As is shown the graph above all three interventions were effective at dropping pain from the beginning. Spinal Manipulative Therapy seemed more effective than medication according to various measures in both acute and subacute neck pain. This means that SMT could be used as an evidence based first line therapy for neck pain. This is substantial because 70% of people will experience neck pain at some point in their lives.
This randomized controlled trial of 272 persons aged 18 to 65 years who had nonspecific neck pain for 2 to 12 weeks was used to compare 12 weeks of chiropractic, medication, or home exercise activities.
The chart above indicates that a chiropractic adjustment had a statistically significant advantage over medication after 8, 12, 26, and 52 weeks, and home exercise was superior to medication at 26 weeks. They both reduced pain equally. Showing that chiropractic and home exercise had similar outcomes at most time points.
The primary measure was participant-rated pain, measured at 2, 4, 8, 12, 26, and 52 weeks. Secondary measures were self-reported disability, global improvement, medication use, satisfaction, general health status (Short Form-36 Health Survey physical and mental health scales), and cervical spine motion.
For the study there were six chiropractors with a minimum of 5 years’ experience who met participants for 15 to 20 minutes and included a brief history and examination of the cervical and thoracic spine followed by an adjustment of areas of the spine with segmental hypomobility by using diversified techniques, including low-amplitude spinal adjustments (a high-velocity type of joint thrust manipulation) and mobilization (a low-velocity type of joint oscillation) based on the findings.
Medication Group
Medications and number of visits were made by the physician on the basis of the participant’s history and response to treatment. Visits lasted 15 to 20 minutes and included a brief history and examination. The first line of therapy was non- steroidal anti-inflammatory drugs, acetaminophen, or both. Unresponsive participants received narcotic medications or muscle relaxants.
HEA Group
Six therapists provided 1 on 1 home exercise with advice in two 1-hour sessions, 1 to 2 weeks apart. The primary focus was simple self- mobilization exercise (gentle controlled movement) of the neck and shoulder joints, including neck retraction, extension, flexion, rotation, lateral bending motions, and scapular retraction, with no resistance. Each program was individualized to the participant’s abilities, tolerance, and activities of daily living. Participants were instructed to do 5 to 10 repetitions of each exercise up to 6 to 8 times per day.
Primary Outcomes
Chiropractic participants experienced reductions of pain of at least 50% in the short term. Longer-term analyses showed similar findings. At 26 and 52 weeks, participant-rated pain improvement favored SMT over medication, but not SMT over HEA or HEA over medication, compared with baseline. The SMT and HEA groups performed similarly on most of the secondary outcomes, although SMT performed better than HEA for satisfaction with care in both the short and long term. Overall, the greatest changes in cervical spine motion were observed in the HEA group.
No evidence-informed first-line therapy for this type of neck pain has been established.
References
1. Coˆte ́ P, Cassidy JD, Carroll L. The Saskatchewan health and back pain survey. The prevalence of neck pain and related disability in Saskatchewan adults. Spine (Phila Pa 1976). 1998;23:1689–98. [PMID: 9704377]
2. Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population: a systematic critical review of the literature. Eur Spine J. 2006;15: 834–48. [PMID: 15999284]
3. Hogg-Johnson S, van der Velde G, Carroll LJ, Holm LW, Cassidy JD, Guzman J, et al; Bone and Joint Decade 2000 –2010 Task Force on Neck Pain and Its Associated Disorders. The burden and determinants of neck pain in the general population: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976). 2008;33:S39- 51. [PMID: 18204398]
4. Guzman J, Haldeman S, Carroll LJ, Carragee EJ, Hurwitz EL, Peloso P, et al; Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Clinical practice implications of the Bone and Joint De- cade 2000–2010 Task Force on Neck Pain and Its Associated Disorders: from concepts and findings to recommendations. Spine (Phila Pa 1976). 2008;33: S199–213. [PMID: 18204393]
5. Riddle DL, Schappert SM. Volume and characteristics of inpatient and am- bulatory medical care for neck pain in the United States: data from three national surveys. Spine (Phila Pa 1976). 2007;32:132–40. [PMID: 17202904]
6. Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data. 2004:1- 19. [PMID: 15188733]
7. Coulter ID, Hurwitz EL, Adams AH, Genovese BJ, Hays R, Shekelle PG. Patients using chiropractors in North America: who are they, and why are they in chiropractic care? Spine (Phila Pa 1976). 2002;27:291–6. [PMID: 11805694] 8. Martin BI, Deyo RA, Mirza SK, Turner JA, Comstock BA, Hollingworth W, et al. Expenditures and health status among adults with back and neck problems. JAMA. 2008;299:656–64. [PMID: 18270354]
9. Coˆte ́ P, van der Velde G, Cassidy JD, Carroll LJ, Hogg-Johnson S, Holm LW, et al; Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. The burden and determinants of neck pain in workers: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976). 2008;33:S60–74. [PMID: 18204402]
10. Coˆte ́ P, Kristman V, Vidmar M, Van Eerd D, Hogg-Johnson S, Beaton D, et al. The prevalence and incidence of work absenteeism involving neck pain: a cohort of Ontario lost-time claimants. Spine (Phila Pa 1976). 2008;33:S192–8. [PMID: 18204392]
Originally published on Medium