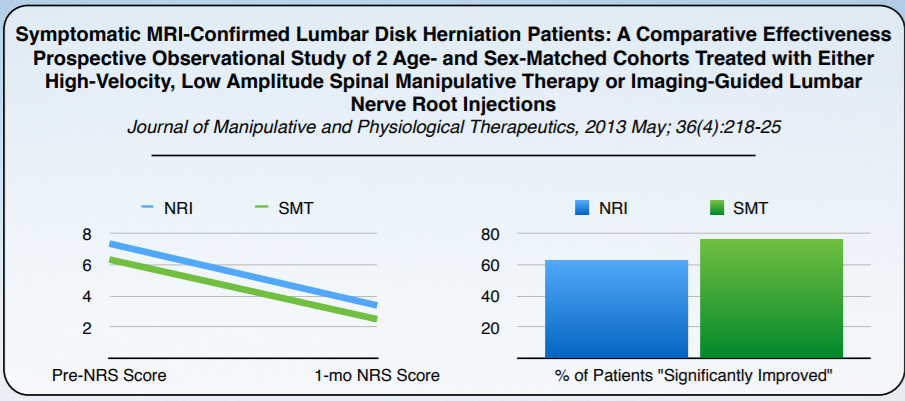
Review of “Symptomatic MRI-Confirmed Lumbar Disk Herniation Patients: A Comparative Effectiveness Prospective Observational Study of 2 Age- and Sex-Matched Cohorts Treated with Either High-Velocity, Low Amplitude Spinal Manipulative Therapy or Imaging-Guided Lumbar Nerve Root Injections Journal of Manipulative and Physiological Therapeutics, 2013 May; 36(4):218–25”
Chances are 7 of your ten friends has had back pain at one point in time.1 Extremely disabling low back pain with leg pain is caused by herniated inter-vertebral disk. A variety of treatment options are available to the patient that can be grouped into 2 categories: surgical and conservative care. Conservative care may include oral medication, corticosteroid and anesthetic infiltrations (nerve root injections [NRIs]), bed rest, exercise therapy, flexion/distraction therapy, and spinal manipulative therapy (SMT).
Chiropractic is More Cost Effective Than Nerve Root Injections
The current standard of care for the 5% of the population with symptomatic lumbar disk herniation is nerve root injection followed by a surgical intervention. Spinal manipulative therapy is controversial all even though evidence shows that improvement with a chiropractic adjustment was higher than those treated with a nerve root injection (NRI). This evidence shows that “spinal manipulation, is a very safe and cost-effective option to treat Lumbar Disk Herniation.” “Both of the treatment groups had significant decreases in their NRS scores at 1 month with a 60% reduction for the Spinal Manipulative Therapy cohort and a 53% reduction for the Nerve Root Injection group.”
This far exceeded the minimum value of 30% required for a clinically meaningful result.24 Although a higher percentage of patients in the SMT group reported being “much better” or “better” (ie, clinically relevant improvement)25,26 on the PGIC scale (76.5% vs 62.7%) at 1 month, this was not statistically significant. “Lumbar NRI’s are a commonly used and accepted treatment option for these patients, whereas lumbar spinal manipulation as a treatment for disk herniation remains controversial among some health care professionals.” The goal of this research is to show that SMT is equally as effective to NRI.
Slipped Discs in Your Back Improved with Chiropractic
Self-reported pain and “improvement” of patients with symptomatic, magnetic resonance imaging — confirmed, lumbar disk herniations improved in both high-velocity, low- amplitude spinal manipulative therapy (SMT) or nerve root injections (NRI).
“Improvement” was reported in 76.5% of SMT patients and in 62.7% of the NRI group. Both groups reported significantly reduced NRS scores at 1 month (P = .0001). Average cost for treatment with SMT was US $558.75 and US $729.61 for NRI. There is no significant difference in outcomes between NRI and SMT for clinically relevant reduction in self- reported pain level and increased global perception of improvement.
This research shows that chiropractic care is both cost effective, clinically significant and needs to be offered as part of the spinal care algorithm. I work closely with nearby clinics offering nerve root injections to ensure that you get the best care possible.
Check out my eBook on Chronic Neck Pain.
References
- van Tulder M, Koes B, Bombardier C. Low back pain. Best Pract Res Clin Rheumatol 2002;16:761–75.
2. Heliovaara M, Impivaara O, Sievers K, et al. Lumbar disc syndrome in Finland. J Epidemiol Community Health 1987; 41:251–8.
3. Heliovaara M, Makela M, Knekt P, Impivaara O, Aromaa A. Determinants of sciatica and low back pain. Spine 1991;16: 608–14.
4. Boden SD, Davis DO, Dina TS, Patronas NJ, Wiesel SW. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 1990;72:403–8.
5. Weber H, Holme I, Amlie E. The natural course of acute sciatica with nerve root symptoms in a double-blind placebo- controlled trial evaluating the effect of piroxicam. Spine 1983; 18:1433–8.
6. Eckel T, Bartynski W. Epidural steroid injections and selective nerve root blocks. Tech Vasc Interv Radiol 2009;12:11–21.
7. Manchikanti L, Boswell MV, Singh V, et al. Comprehensive evidence-based guidelines for interventional techniques in the management of chronic spinal pain. Pain Physician 2009;12: 699–802.
8. Peterson C, Hodler J. Evidence-based radiology (part 1): is there sufficient research to support the use of therapeutic injections for the spine and sacroiliac joints? Skeletal Radiol 2010;39:5–9.
9. Roberts S, Willick S, Rho M, Rittenberg J. Efficacy of lumbosacral transforaminal epidural steroid injections: a systematic review. PMR 2009;1:657–68.
10. Abdi S, Datta S, Trescot A, et al. Epidural steroids in the management of chronic spinal pain: a systematic review. Pain Physician 2007;10:185–212.
11. Datta S, Everett C, Trescot A, et al. An updated systematic review of the diagnostic utility of selective nerve root blocks. Pain Physician 2007;10:113–28.
12. Assendelft WJJ, Morton SC, Yu EI, Suttorp MJ, Shekelle PG. Spinal manipulative therapy for low back pain: a meta- analysis of effectiveness relative to other therapies. Ann Intern Med 2003;138:871–81.
13. Oiphant D. Safety of spinal manipulation in the treatment of lumbar disc herniations: a systematic review and risk assessment. J Manipulative Physiol Ther 2004;27:197–210.
14. Santilli V, Beghi E, Finucci S. Chiropractic manipulation in the treatment of acute back pain and sciatica with disc protrusion: a randomized double-blind clinical trial of active and simulated spinal manipulations. Spine J 2006;6:131–7.
15. Luijsterburg P, Verhagen A, Ostelo RW, van Os TA, Peul WC, Koes BW. Effectiveness of conservative treatments forthe lumbosacral radicular syndrome: a systematic review. EurSpine J 2007;16:881–99.
16. Lawrence DJ, Meeker W, Branson R, et al. Chiropractic management of low back pain and low back-related leg complaints: a literature synthesis. J Manipulative Physiol Ther 2008;31:659–74.
17. Leininger B, Bronfort G, Evans R, Reiter T. Spinal manipulation or mobilization for radiculopathy: a systematic review. Phys Med Rehabil Clin N Am 2011;22:105–25.
18. McMorland G, Suter E, Casha S, du Plessis SJ, Hurlbert RJ. Manipulation or microdiskectomy for sciatica? A prospective randomized clinical study. J Manipulative Physiol Ther 2010; 33:576–84.
19. Lisi AJ, Holmes EJ, Ammendolia C. High-velocity low amplitude spinal manipulation for symptomatic lumbar disk disease: a systematic review of the literature. J Manipulative Physiol Ther 2005;28:429–42.
20. Peterson CK, Bolton J, Humphreys BK. Predictors of improvement in patients with acute and chronic low back pain undergoing chiropractic treatment. J Manipulative Physiol Ther 2012;35:525–33.
21. Peul WC, van Houwelingen HC, van den Hout WB, et al. Surgery versus prolonged conservative treatment for sciatica. N Engl J Med 2007;356:2245–56.
22. Tinetti ME, Studenski SA. Comparative effectiveness re- search and patients with multiple chronic conditions. N Engl J Med 2011;364:2478–81.
23. Fischer D, Stewart AL, Bloch DA, Lorig K, Laurent D, Holman H. Capturing the patient’s view of change as a clinical outcome measure. JAMA 1999;282:1157–62.
24. Ostelo RW, Deyo RA, Stratford P, et al. Interpreting change scores for pain and functional status in low back pain. Spine 2008;33:90–4.
25. Hurst H, Bolton J. Assessing the clinical significance of change scores recorded on subjective outcome measures. J Manipulative Physiol Ther 2004;27:26–35.
26. Newell D, Bolton JE. Responsiveness of the Bournemouth questionnaire in determining minimal clinically important change in subgroups of low back pain patients. Spine 2010; 35:1801–6.
Article originally published on Medium.